Proton Pump Inhibitors: Helpful Therapy, But Worth a Second Look
Proton pump inhibitors (PPIs) are among the most commonly prescribed medications in the United States—and for good reason. They are highly effective at reducing stomach acid and treating conditions like GERD, peptic ulcer disease, and esophagitis. For many patients, they provide significant relief and protect against serious complications.
However, as with any widely used medication, long-term and “prolific” use deserves thoughtful review—especially when it comes to kidney health.
Why the Concern About PPIs?
Over the past decade, research has raised awareness about several potential side effects associated with prolonged PPI use. While most patients tolerate these medications well, it’s important to understand some of the possible risks:
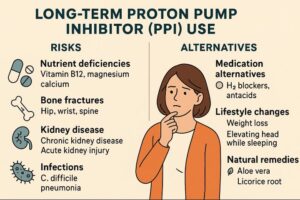
1. Low Magnesium Levels (Hypomagnesemia)
PPIs can, in some cases, reduce magnesium absorption in the gut. Low magnesium may lead to symptoms such as muscle cramps, fatigue, or even heart rhythm disturbances in more severe cases. This tends to occur after long-term use rather than short courses.
2. Risk of B12 deficiency,
Long-term PPI use has been associated with a small increased risk of vitamin B12 deficiency due to reduced stomach acid affecting absorption, usually after several years of therapy. Some studies also show a modest association with increased fracture risk, likely related to altered calcium absorption and overall bone metabolism. Overall, the absolute risk is low, and these effects are generally preventable and manageable with monitoring and appropriate supplementation.
3. Tolerance and Dependence
Although PPIs do not cause “addiction” in the traditional sense, the body can adapt to acid suppression. Over time, patients may feel like they need continued therapy, and stopping suddenly can lead to a rebound increase in acid production.
4. Kidney Concerns, Including Interstitial Nephritis and CKD
One of the more important kidney-related side effects linked to PPIs is acute interstitial nephritis (AIN)—an inflammatory reaction within the kidneys. This is not common, but it is well-documented and important to recognize.
AIN can occur days to months after starting a PPI, and in many cases, symptoms are subtle or even absent. When symptoms do occur, they may include:
- Fatigue
- Nausea
- Decreased urine output
- Occasionally rash, fever, or joint aches
Often, the first sign is simply a rise in creatinine on routine lab work.
In terms of frequency, AIN is considered rare—only a small percentage of patients taking PPIs will ever develop this condition. However, it matters because:
- It is one of the main pathways by which PPIs can affect kidney function
- If recognized early and the medication is stopped, kidney function often improves
- If missed or prolonged, it can lead to permanent kidney damage or progression to chronic kidney disease
Beyond AIN, some observational studies have shown an association between long-term PPI use and an increased risk of chronic kidney disease (CKD). It’s important to emphasize that this is an association—not a direct cause-and-effect relationship in most cases.
Putting the CKD Risk Into Perspective
When patients hear “increased risk,” it can sound alarming. But context matters.
For many individuals, the additional risk associated with PPI use is relatively small. One way to think about it is similar to a low-probability event—something like 1 out of 100 patients over time (depending on the study and population).
In other words:
- The vast majority of patients will not develop CKD from PPIs
- But a small increased risk may exist, particularly with long-term use
For patients who already have chronic kidney disease, we take a more cautious and individualized approach. In these cases:
- We review whether the PPI is still necessary
- We consider the lowest effective dose
- We monitor kidney function more closely
- We weigh risks and benefits in collaboration with both a nephrologist and a gastroenterologist
Can an H2 Blocker Be Used Instead?
If symptoms can be controlled with a different class of medication—such as an H2 blocker (e.g., famotidine)—that is often preferred for long-term use due to a more favorable side effect profile.
That said, PPIs are sometimes clearly the best option. For example:
- Severe GERD
- Barrett’s esophagus
- History of gastrointestinal bleeding
- High-risk ulcer prevention
In these situations, the benefit of a PPI often outweighs the relatively small potential risks.
Don’t Stop PPIs Abruptly
One of the most common issues we see is patients stopping their PPI “cold turkey.”
This can lead to rebound acid hypersecretion, where the stomach temporarily produces more acid than before. Symptoms can actually feel worse than the original condition, leading patients to restart the medication and feel “dependent” on it.
A better approach is:
- Gradual dose reduction (tapering)
- Transitioning to an H2 blocker if appropriate
- Using lifestyle modifications (diet changes, weight management, avoiding late meals)
This process should be guided by your healthcare provider to ensure comfort and safety.
The Bottom Line
PPIs are effective and often necessary medications—but like all therapies, they should be used thoughtfully.
- The risk of kidney disease is real but relatively low
- Acute interstitial nephritis is rare but important to recognize early
- Patients with existing CKD should have individualized decision-making
- Alternatives like H2 blockers are considered when appropriate
- Abrupt discontinuation should be avoided
At CT Kidney & Hypertension Specialists, we work closely with patients and their care teams to balance symptom control with long-term kidney health. If you’re taking a PPI and have concerns, it’s worth a conversation—not a sudden change.